Cardiovascular System (Heart)
|
Content
Circulatory System
Functions of the Heart
Blood flow Through the Heart
Cardiac Muscle Cells
Intrinsic Conduction System
Cardiac impulse
Excitation-Contraction
Conduction Pathway
Electrocardiogram
Cardiac Cycle
Heart Sounds
Cardiac Output
Factors Affecting Cardiac Output
-- Preload
-- --Contractility
-----Afterload
Regulation of the Heart
Primary control factors of the heart
Congestive Heart Failure
Circulatory System
The parts of the circulatory system include:
- Heart
- Serves as pump that establishes the pressure gradient needed for blood to flow to tissues
- Blood Vessels
- Passageways through which blood is distributed from heart to all parts of body and back to heart
- Blood
- Transport medium within which materials being transported are dissolved or suspended
|
Functions of the Heart
- Generating blood pressure to produce a gradient that pushes blood through the vascular system
- Routing blood, ensuring one-way blood flow, separates pulmonary and systemic circulations
- Regulating blood supply - changes in contraction rate and force match blood delivery to changing metabolic needs
|
 |
| |
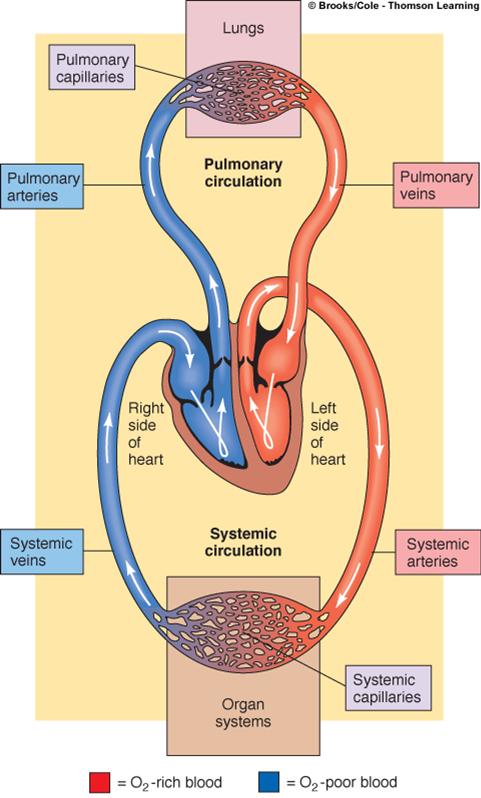 |
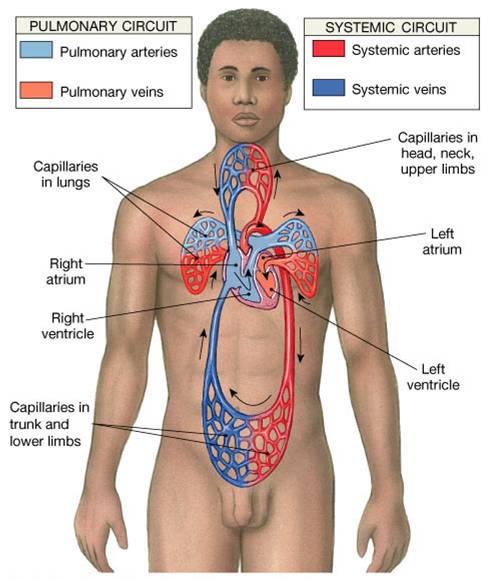
Pulmonary Circulation
- Closed loop of vessels carrying blood between heart and lungs
Systemic Circulation
- Circuit of vessels carrying blood between heart and other body systems
|
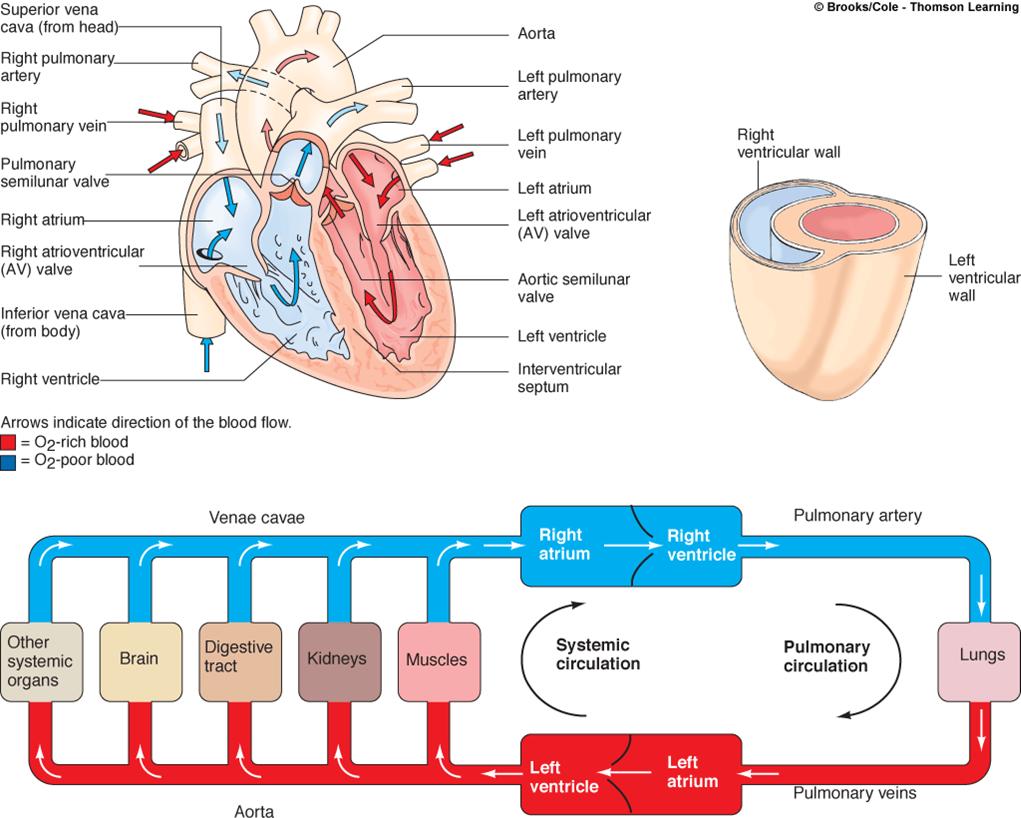
Blood flow Through the Heart
1. Superior/Inferior vena cava and coronary sinus
2. Rt Atrium
3. Tricuspid valve
4. Rt ventricle
5. Pulmonary semilunar valve
6. Pulmonary trunk
7. Right and left pulmonary arteries
8. Lungs
7. Pulmonary veins
8. Lt atrium
9. Bicuspid valve (mitral)
10. Lt ventricle
11. Aortic semilunar valve
12. Ascending aorta
13. Coronary arteries
14. Arch of aorta
 Click here for an animation that summarizes the flow of blood through the heart. Click here for an animation that summarizes the flow of blood through the heart.
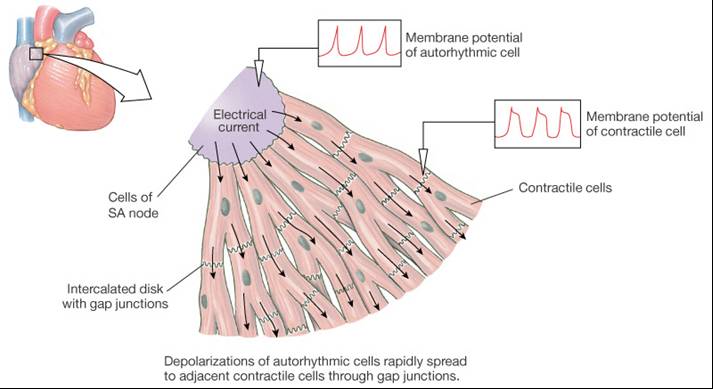
Cardiac Muscle Cells
- Autorhythmic cells
- 1% of cardiac muscle cells
- do not contract
- generate and conduct action potentials
- membrane potential “never rests”
- Contractile cells
- 99% of cardiac muscle cells
- do mechanical work of pumping
- normally do not produce action potentials
- have a different looking action potential fro other nerve cells due to calcium channels
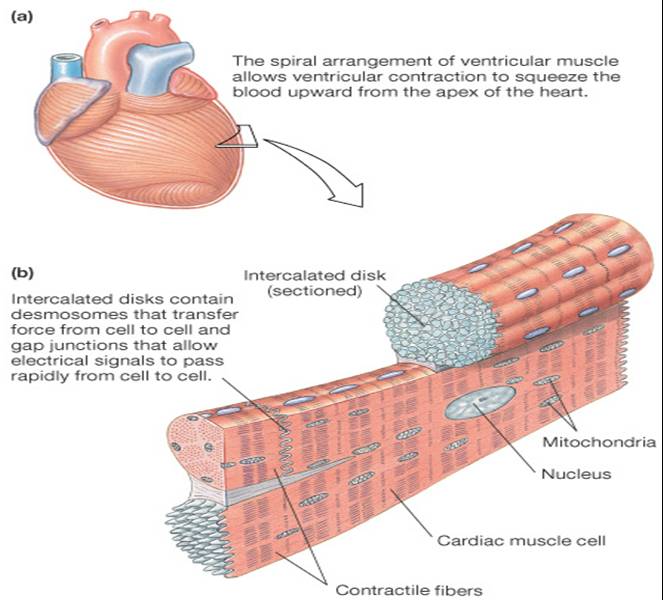
Cardiac Cell Histology
- Intercalated discs allow branching of the myocardium
- Gap junctions (instead of synapses)
- Have fast cell to cell signals
- Have m any mitochondria
- Have large T-tubules
|
Intrinsic Conduction System
- Autorhythmic cells:
- Initiate action potentials
- Have “drifting” resting potentials called pacemaker potentials
- membrane slowly depolarizes “drifts” to threshold, initiates action potential, membrane repolarizes to -60 mV.
- Use calcium influx (rather than sodium) for rising phase of the action potential
|
 |
Autorhythmic cells depolarize spontaneously but at different rates:
Sinoatrioal (SA) node intrinsic rate |
70-80 |
Atrioventricular (AV) node |
40-60 |
Atrioventricular bundles |
20-40 |
Purkinje fibers |
20-40 |
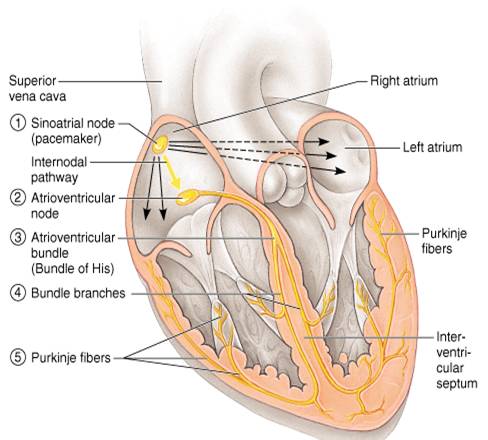
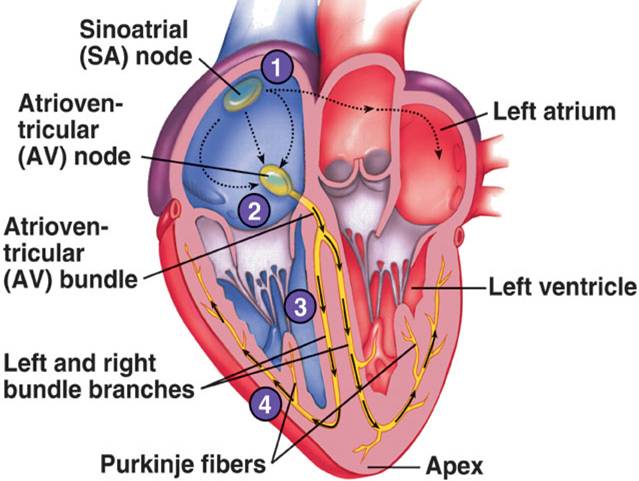
Sinoatrial (SA) Node
- Control the rest of the heart
- Allow the atria to contract first then the ventricles contract
- They act as a pacemaker and a conduction system
- Initiates an action potential which travels throughout heart down to the atrioventricular (AV) node, which slows down the AP before traveling to the atrioventricular bundle (bundle of His) and splits into the R/L bundle branches which spread into conduction myofibers (Purkinje fibers).
 Click here for an animation on the conduction system of the heart. Click here for an animation on the conduction system of the heart.
 The animation is followed by practice questions. The animation is followed by practice questions.
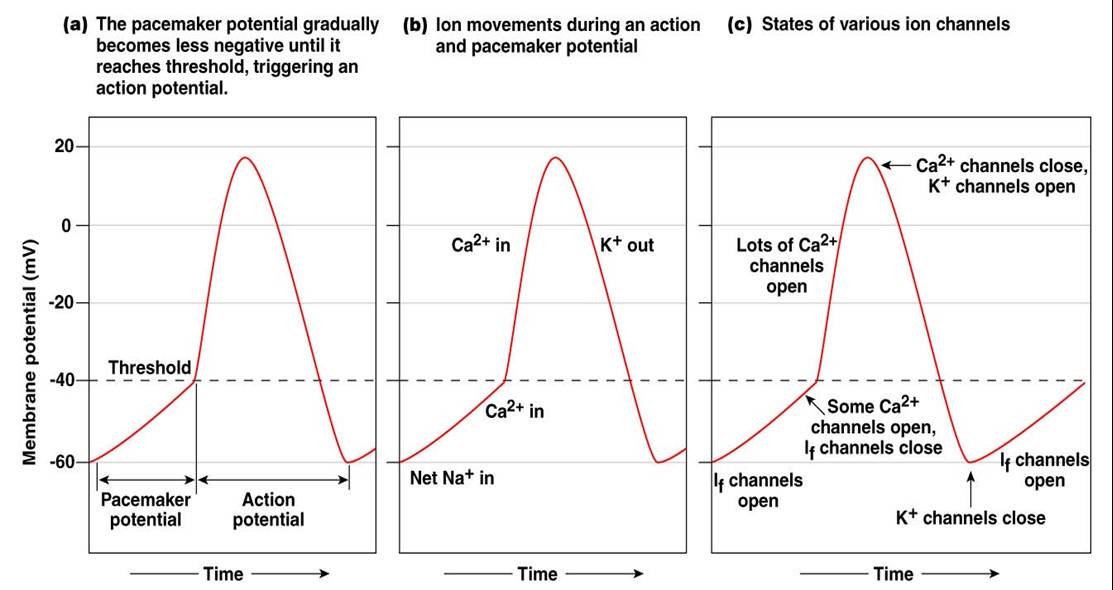
Pacemaker Potential
- Membrane slowly depolarizes “drifts” to threshold
- Initiates action potential
- Membrane repolarizes to -60 mV

Cycle
1. Normal RMP at -60mV
2. Decreased efflux of K+, membrane permeability decreases between APs, they slowly close at negative potentials
3. Constant influx of Na+, no voltage-gated Na + channels
4. Gradual depolarization because K+ builds up and Na+ flows inward
5. As depolarization proceeds Ca++ channels (Ca2+ T) open before threshold is reached
6. Slow influx of Ca++ further depolarizes bringing to threshold (-40mV)
7. At threshold sharp depolarization due to activation of Ca2+ L channels allow large influx of Ca++
8. Falling phase at about +20 mV the Ca-L channels close, voltage-gated K channels open
9. Repolarization due to normal K+ efflux
10. At -60mV K+ channels close
|
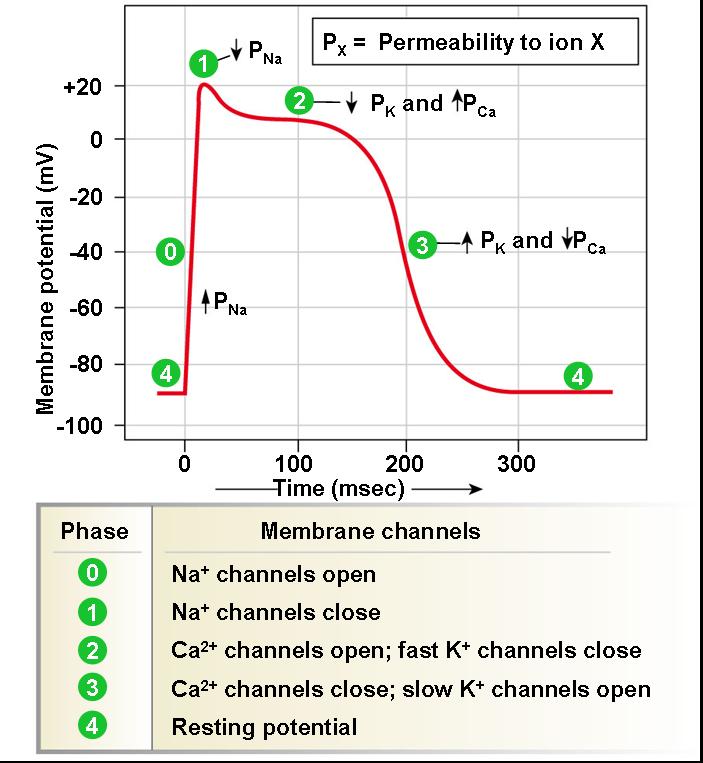
Action Potential of Contractile Cardiac Cells
- Begins with rapid depolarization
- Rapid, partial early repolarization, prolonged period of slow repolarization which is plateau phase
- Rapid final repolarization phase
|
 |
Cardiac impulse
A wave of depolarization that begins in the pacemaker and spreads over the heart (it precedes contraction)
Summary
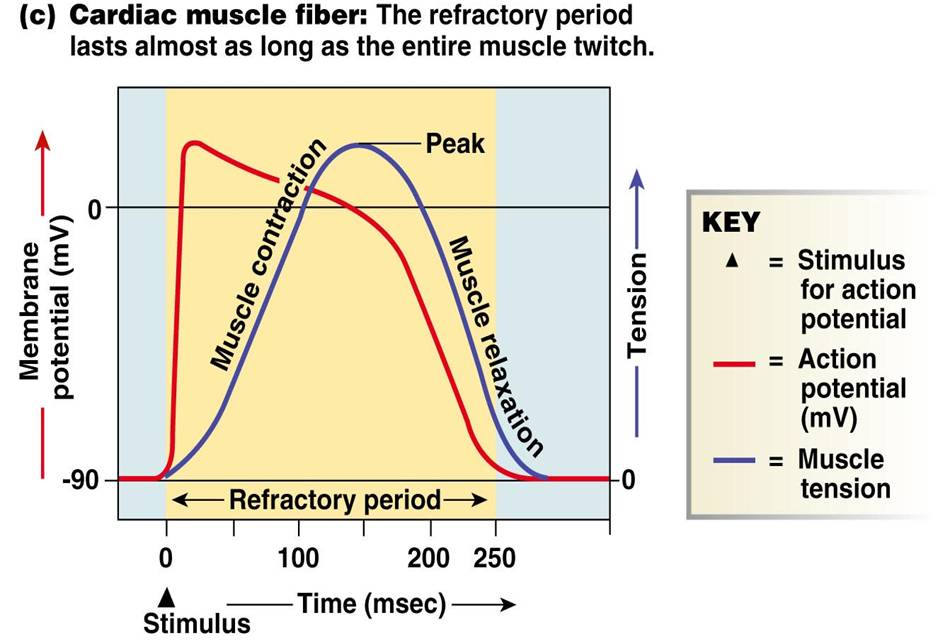
- The resting membrane potential of the cardiac muscle fiber is -90 mV inside the cell
- The resting membrane potential is created by actively pumping sodium ions (Na+) out of the fiber
- An action potential stimulates the contractile fibers to depolarize - voltage gated channels in the membrane to open allowing sodium ions to flow back in the cytosol
- At +30 mV, the Na+ channels close decreasing potential, however the membrane then enters a plateau by allowing calcium ion (Ca++ ) channels to open causing a them to also flow inside the cytosol
- in addition the fast potassium ion (K+) channels close reducing their effux
- The combined build up of Ca++ and K+ ions causes a delay of up to 250 milliseconds (.25 sec)
- After the plateau phase the fiber repolarizes by allowing K+ions to flow out of the cytosol and at the same time the Ca++channels close
- The refractory period of a cardiac fiber is longer than the contraction itself, as a result tetanus cannot occur
Why a longer AP in cardiac contractile fibers?
- Don’t want summation and tetanus in our myocardium.
- A myocardium in a state of tetanus ceases to be a pump
- Long refractory period occurs in conjunction with prolonged plateau phase, summation and tetanus of cardiac muscle is impossible
- Ensures alternate periods of contraction and relaxation which are essential for pumping blood
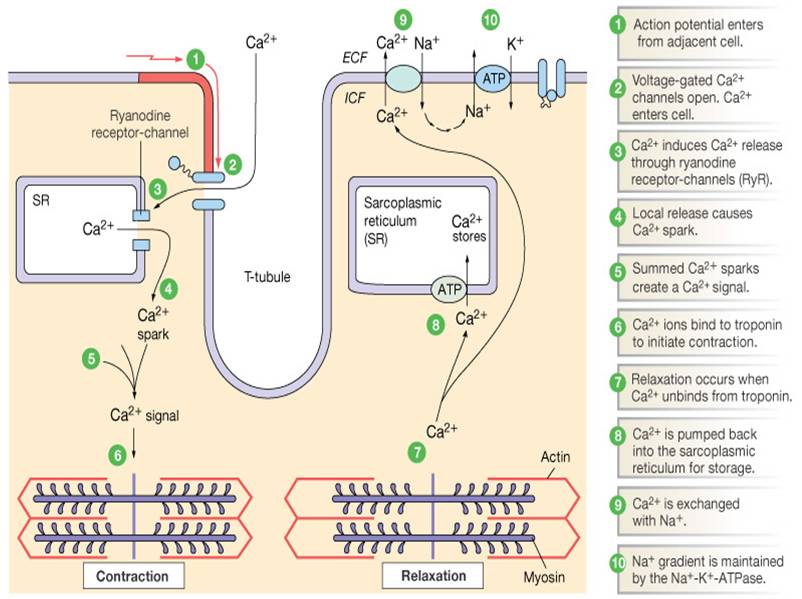
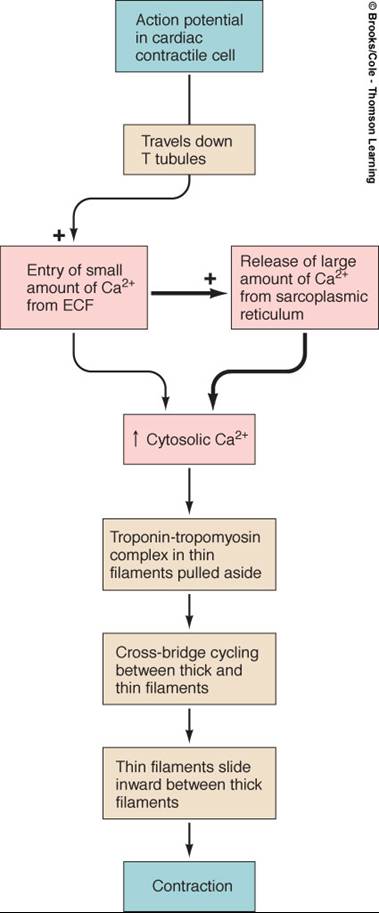
Excitation-Contraction Coupling in Cardiac Contractile Cells
- Ca++ entry through L-type channels in T-tubules triggers larger release of Ca++ from sarcoplasmic reticulum
- Ca++ induced Ca++ release leads to cross-bridge cycling and contraction
Electrical Signal Flow - Conduction Pathway
- Cardiac impulse originates at SA node
- Action potential spreads throughout right and left atria
- Impulse passes from atria into ventricles through AV node (only point of electrical contact between chambers
- Action potential briefly delayed at AV node (ensures atrial contraction precedes ventricular contraction to allow complete ventricular filling)
- Impulse travels rapidly down interventricular septum by means of bundle of His
- Impulse rapidly disperses throughout myocardium by means of Purkinje fibers
- Rest of ventricular cells activated by cell-to-cell spread of impulse through gap junctions
Electrocardiogram (ECG or EKG)
- Is a record of overall spread of electrical activity through heart
- Represents:
- Recording part of electrical activity induced in body fluids by cardiac impulse that reaches body surface
- Not direct recording of actual electrical activity of heart
- Recording of overall spread of activity throughout heart during depolarization and repolarization
- Not a recording of a single action potential in a single cell at a single point in time
- Comparisons in voltage detected by electrodes at two different points on body surface, not the actual potential
- Does not record potential at all when ventricular muscle is either completely depolarized or completely repolarized
- Wave = upwards or downwards deflection
Segment = flat portion between waves
Interval = often a wave plus a segment
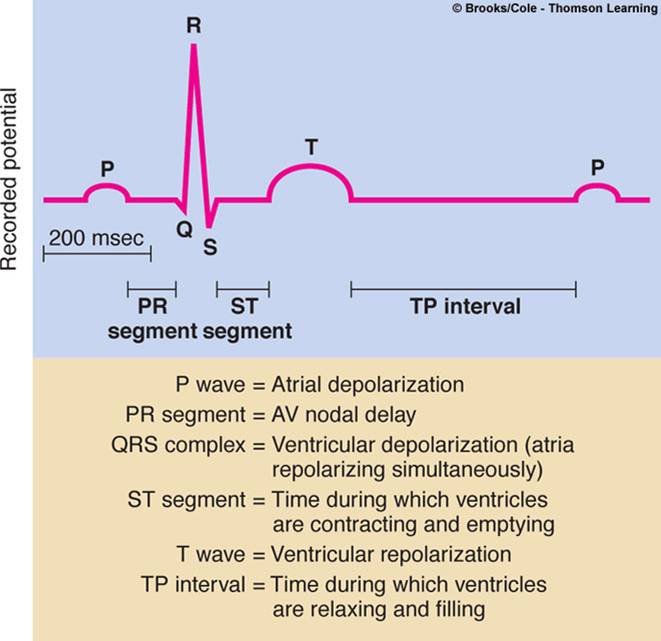
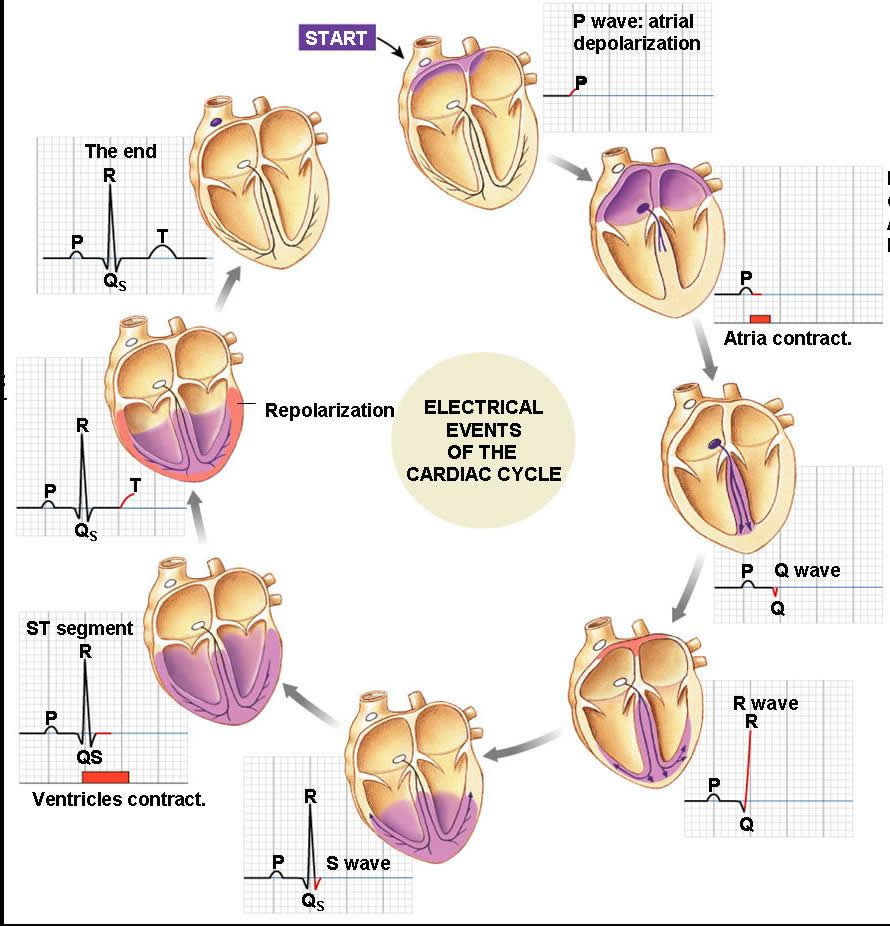
- P wave - atrial depolarization
- QRS complex - ventricular depolarization
- T wave - ventricular repolarization
- PR interval - conduction time from the end atrial depolarization to the onset ventricular depolarization
- ST interval - time when ventricular fibers are fully depolarized.
- TP interval – when the heart muscle is completely at rest and ventricular filling is taking place
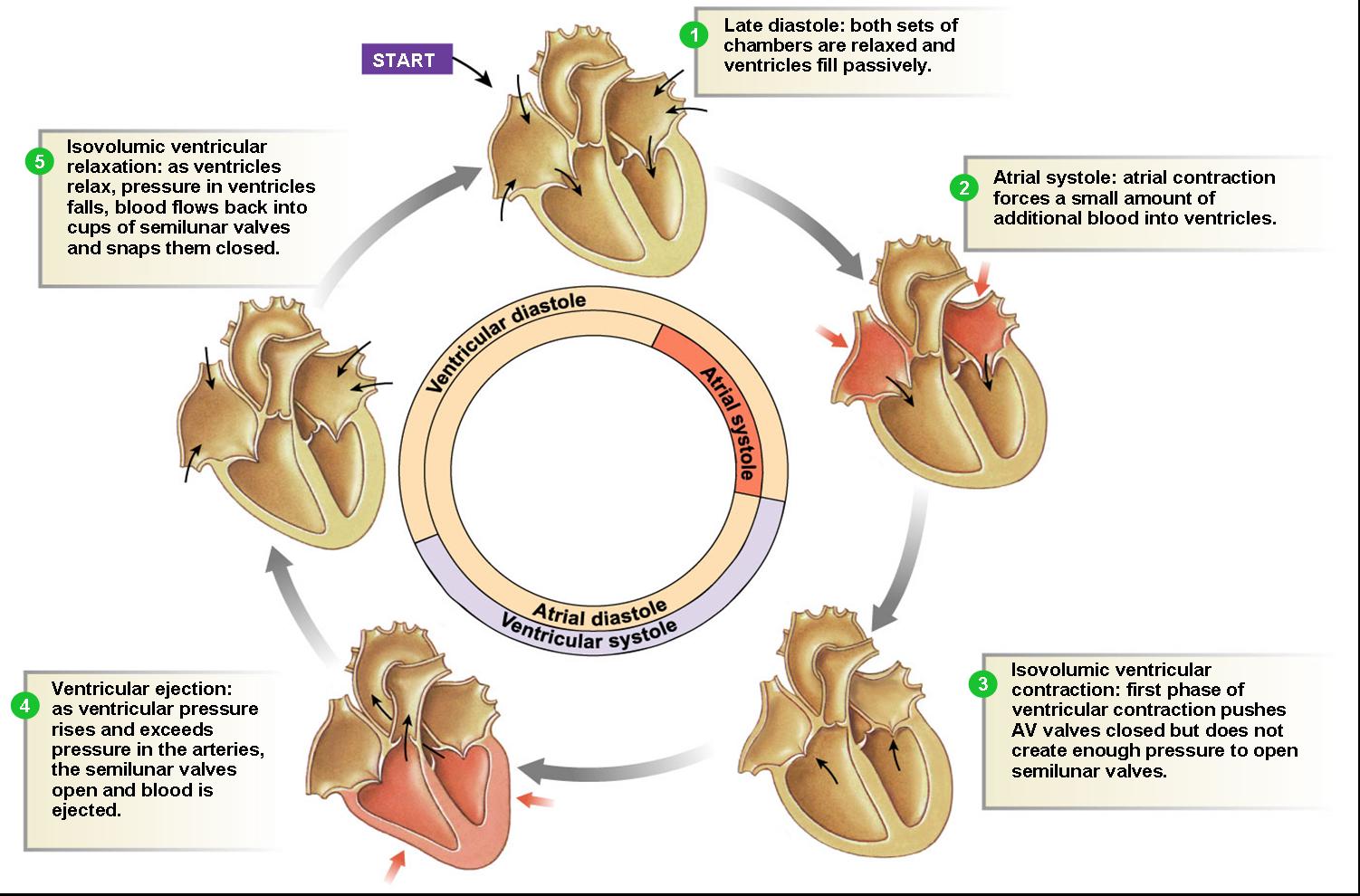
Cardiac Cycle - Filling of Heart Chambers
- Heart is two pumps that work together, right and left half
- Repetitive contraction (systole) and relaxation (diastole) of heart chambers
- Blood moves through circulatory system from areas of higher to lower pressure.
- Contraction of heart produces the pressure
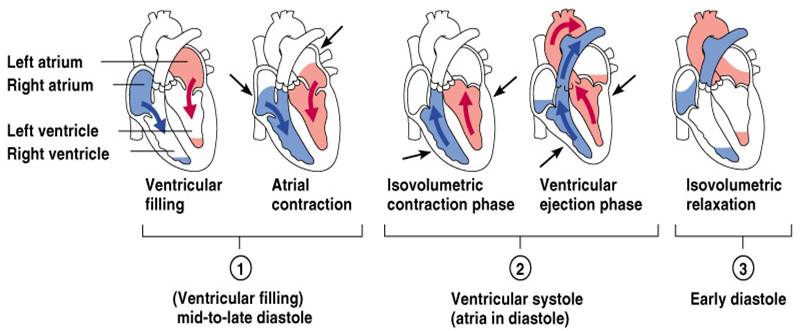
- Atrial Systole 0.1 sec
- Atria contract
- AV valves open
- SL valves closed
- Ventricles relaxed (in diastole)
- Active Ventricular Filling
- When AV valves open blood flows into the ventricles
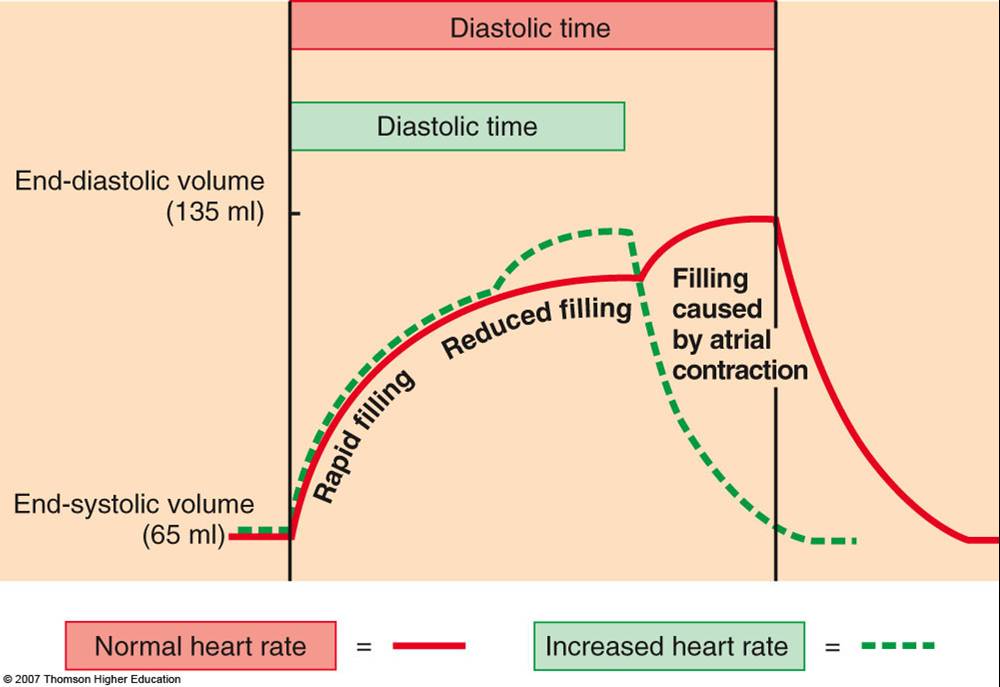
- The ventricles are completely filled when the atria contract forcing more (30ml) of blood inside the ventricles
- The blood volume is now 130ml and is called the end diastolic volume
- Ventricular Systole
- 0.3 sec
- when the action potential from the SA node passes through the AV node and into the ventricles it causes depolarization and ventricular contraction
- Isovolumetric Contraction Phase
- ventricles begin to contract
- AV valves close
- SL valves still closed
- atria in diastole, pressure in ventricles increases
- Ejection Phase
- Pressure inside rises and forces open the semilunar valves and the blood is ejected into arteries
- The blood volume remaining in the heart after ventricular ejection, about 60ml, is called the end systolic volume.
- Relaxation
- Ventricles relax (diastole - T wave initiated)
- Isovolumetric Ventricular Relaxation and Passive Ventricular Filling
- 0.4 sec)
- atria and ventricles in diastole
- pressure in ventricles decrease and blood back flows from the aorta and pulmonary vein closing the semilunar valves
- At end of isometric ventricular relaxation, ventricular pressure drops sufficiently the AV valves open allowing blood to leave the atria.
Click here for an animation on the cardiac cycle of the heart.
The animation is followed by practice questions. Click here for even more practice questions.
|
|
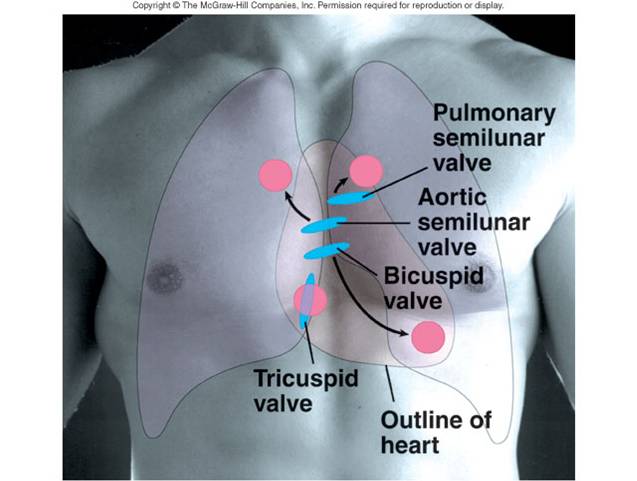
Heart Sounds
- Act of listening is called auscultation
- There are three heart sounds primarily created by heart valves closing and blood turbulence
- Lubb - Atrioventricular valves close
Dupp - Semilunar valves close
|
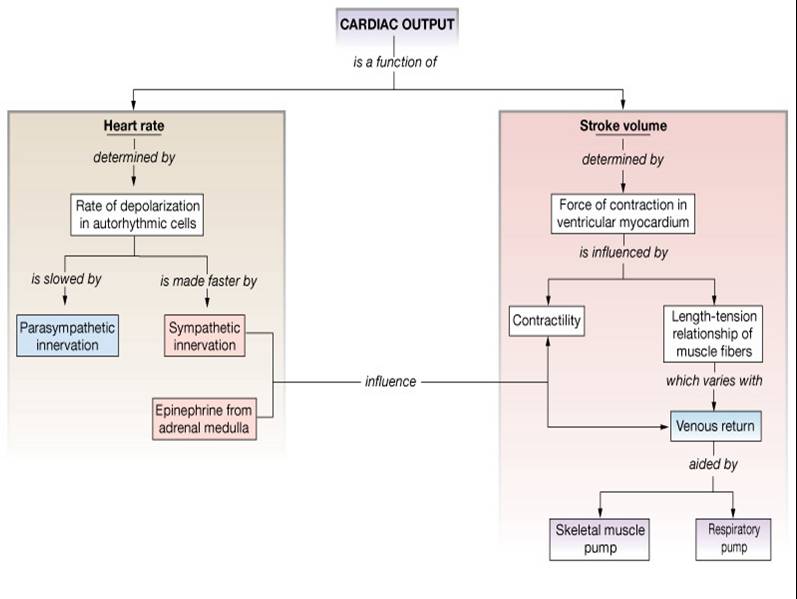
Cardiac Output (CO) and Reserve
Cardiac output (CO) is the amount of blood ejected by the left ventricle into the aorta per minute.
CO = stroke volume (amount of blood ejected with each systole) x beats per minute.
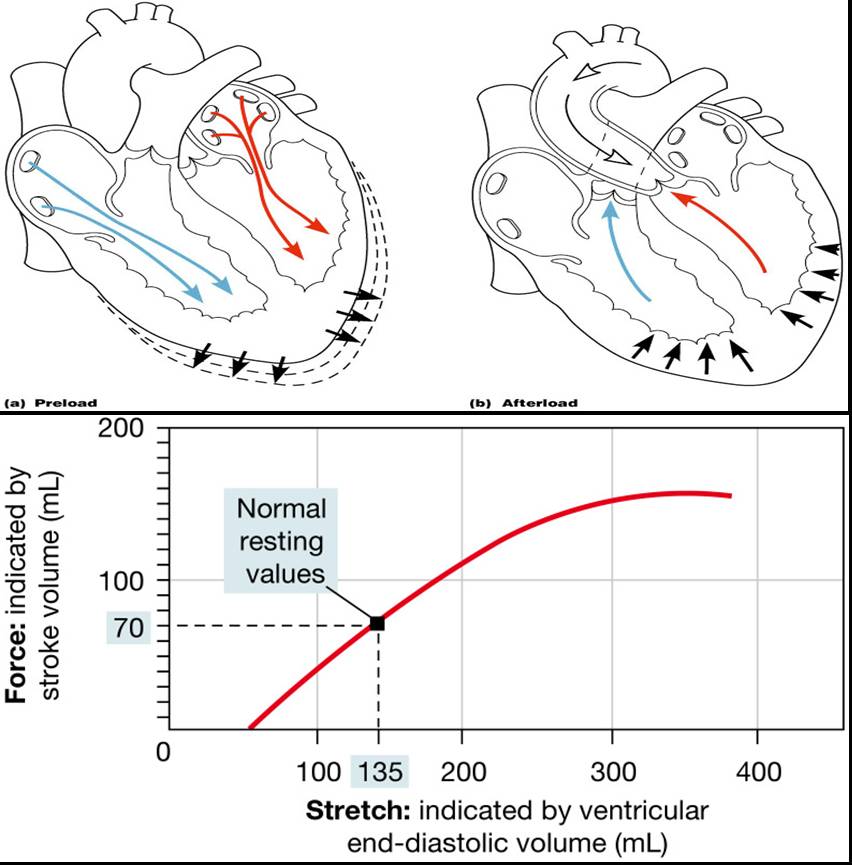
End Diastolic Volume (EDV) – End Systolic Volume (ESV) = SV ex. 135- 65 = 70 ml, Residual (about 50%)
Stroke Volume (SV) is the amount of blood pumped out by a ventricle with each beat
Cardiac Output ~ 5L: (70 beats/m X 70 ml/beat = 4900 ml)
Cardiac Reserve - Cardiac reserve is the difference between resting and maximal CO - ratio between the maximum cardiac output a person can achieve and the cardiac output at rest. Normally the figure is four to five times the resting output. maximum CO ~ 25 L/min
Factors Affecting Cardiac Output
- Chronotropes (ANS) affect heart rate
- Inotropes affect contractility (stroke volume)
|
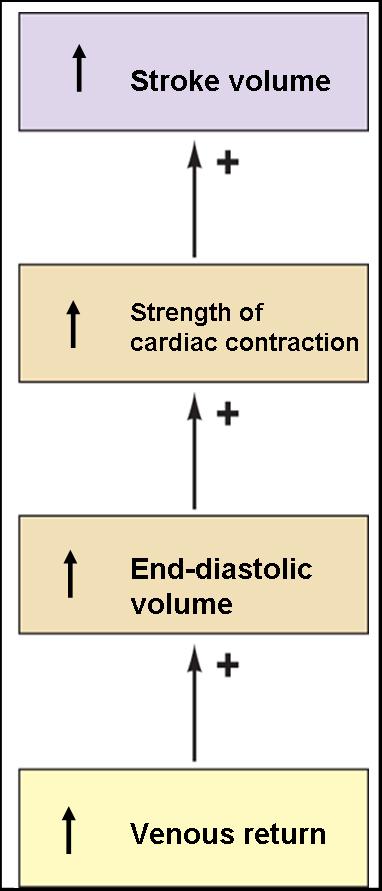
1. Preload Stretch - Frank - Starling law - the greater the stretch on cardiac fibers just before they contract (draws myosin fibers closer together) increases their force of contraction, the more blood is ejected from the ventricle the heart is filled during diastole the greater the force of contraction
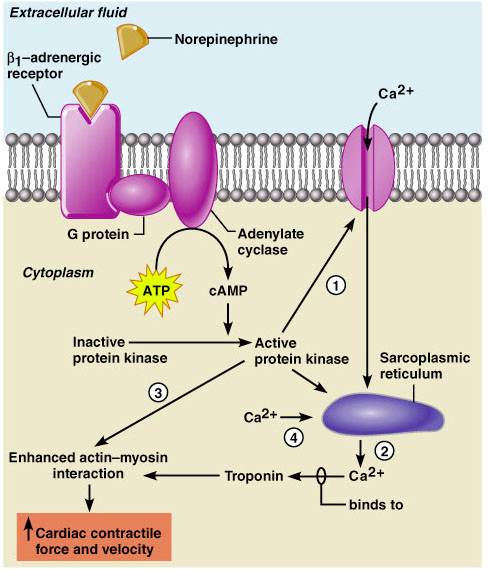
2. Contractility - strength of a contraction at any give preload. Substances that increase contractility (positive inotropic agents) include hormones (glucagons, thyroxine), catecholemines (epinephrine and norepinephrine), drugs (digitalis) and increased calcium concentration in the extracellular fluid.
3. Afterload - the pressure in the large arteries leaving the heart that must be overcome before the aortic semilunar valve can open. Increased afterload results in decreased stroke volume. |
|
Preload, or degree of stretch, of cardiac muscle cells before they contract is the critical factor controlling stroke volume
Slow heartbeat and exercise increase venous return to the heart, increasing SV
Blood loss and extremely rapid heartbeat decrease SV
Contractility and Norepinephrine - sympathetic stimulation releases norepinephrine and initiates a cyclic AMP second-messenger system
Regulation of the Heart
Intrinsic regulation: Results from normal functional characteristics - Starling’s law of the heart
Frank- Starling’s Law
- Preload, or degree of stretch, of cardiac muscle cells before they contract is the critical factor controlling stroke volume
- Slow heartbeat and exercise increase venous return to the heart, increasing SV
- Blood loss and extremely rapid heartbeat decrease SV
Extrinsic regulation:
- Involves neural and hormonal control – Autonomic Nervous system
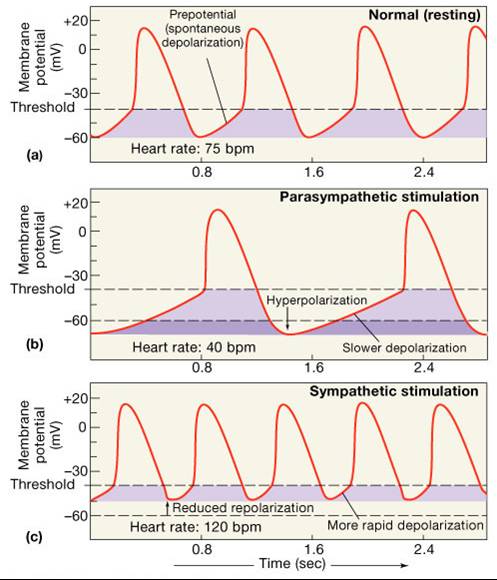
- Sympathetic stimulation – “Fight or Flight"supplied by cardiac nerves, increases heart rate and force of
contraction
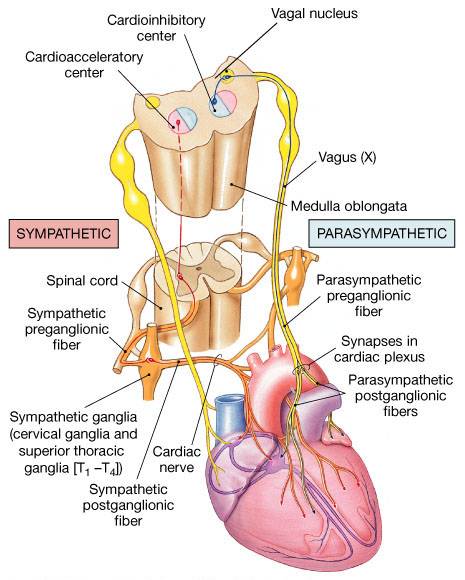
- Sympathetic nerves include the cardiac accelerator nerves which extend out to the SA node, AV node and
portions of the myocardium, releasing norepinephrine and epinephrine from adrenal medulla which increases
heart rate and contractility
- Parasympathetic stimulation – normally dominates – “resting” heart rate
- Parasympathetic nerves include the right and left Vagus (X) nerves. These fibers innervate the SA node, AV
node and the atrial myocardium, releasing acetylcholine which decreases heart rate.
There is always a balance between sympathetic and parasympathetic stimulation of the heart, but the parasympathetic dominates at rest.
Primary control factors of the heart
- Hormones - adrenal hormones (epinephrine and norepinephrine) and thyroid hormones.
- Ions - relative ion concentrations of K+ , Na+ , and Ca++ can also effect heart rate and contractility.
- Gases - oxygen, carbon dioxide
- pH - acidosis, alkalosis
- Age
- Gender
- Fitness
- Body temperature
Medulla Oblongata Centers Affect Autonomic Innervation
- Cardio-acceleratory center activates sympathetic neurons
- Cardio-inhibitory center controls parasympathetic neurons
- Receives input from higher centers, monitoring blood pressure and dissolved gas concentrations
Congestive Heart Failure (CHF)
CHF is caused by:
- Coronary atherosclerosis
- Persistent high blood pressure
- Multiple myocardial infarcts
- Dilated cardiomyopathy (DCM)
Top ------- Main Page
|